
Tuesday, August 20, 2013
Expanding Team Coverage
I wanted to write today and thank the new schools that have offered to have me as part of their already excellent medical teams. I'll be working with a stellar group of doctors and trainers to provide orthopedic and sports medicine coverage at Jeffersonville, Clarksville, Providence, Charlestown, and North Harrison High Schools for the upcoming scholastic season. This is in addition to continuing my work with Indiana University Southeast, the University of Louisville, and Waggener High School. Providing care for scholastic athletes is one of the highlights of my career and I look forward to a successful and healthy season for all the competitors. Thanks to everyone at these institutions for having me as part of the team.
Thursday, August 15, 2013
I tore my ACL
The words above are amongst the most dreaded that can be spoken by any patient, be it a scholastic athlete, weekend warrior, or a work injury. Although the widespread attention this injury and its treatment have garnered from the coverage of college and professional athletes who have suffered it, there is often a significant amount of fear and uncertainty when dealing with the diagnosis, management, and recovery from this injury. The following post will go over this and hopefully provide a primer for patients and their families’ as they begin the road to recovery.
What is your ACL?
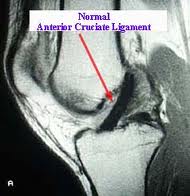
 The ACL, or anterior cruciate ligament, is one of four stabilizing ligaments of the knee. It is located within the knee joint and when torn, can leave the patient with the inability to perform activities that require cutting, pivoting, and a change of direction. Heavy lifting, climbing, and other job activities can be difficult as well. Walking, swimming, and other straight ahead and low impact activities are less often affected by this injury. ACL tears primarily occur via noncontact mechanisms. That is, an athlete will often be changing direction or landing when the injury occurs. These moments can be quite painful and patients will often feel or hear a pop, followed by rapid swelling of the knee and the inability to bear weight on the leg.
The ACL, or anterior cruciate ligament, is one of four stabilizing ligaments of the knee. It is located within the knee joint and when torn, can leave the patient with the inability to perform activities that require cutting, pivoting, and a change of direction. Heavy lifting, climbing, and other job activities can be difficult as well. Walking, swimming, and other straight ahead and low impact activities are less often affected by this injury. ACL tears primarily occur via noncontact mechanisms. That is, an athlete will often be changing direction or landing when the injury occurs. These moments can be quite painful and patients will often feel or hear a pop, followed by rapid swelling of the knee and the inability to bear weight on the leg.
How do I know if I tore it?
Most ACL tears will have the typical history above. I recommend anyone with that history to be evaluated by a physician in short time. That evaluation will focus on several things. First the stability of the knee will be tested on physical examination. This can also diagnose other ligament tears that can be associated with ACL tears. X-rays are helpful to rule out other injuries as well. Commonly this evaluation will result in an MRI, or magnetic resonance image, being ordered. This test, which does not involve radiation, will evaluate the soft tissue, cartilage, and bone of the knee with higher detail than an x-ray. When this information is available, your physician will be able to provide a complete diagnosis and treatment plan.


What’s Next?
At this point the treatment plan becomes very individualized. Every ACL tear is different in the amount of pain and instability a patient will suffer from. Different physical demands also go into determining the best way to treat a tear. In general, the younger and higher demand that a patient’s sport, job, or daily activities require, the more likely a surgical option is to be recommended. Associated injuries like meniscus and cartilage tears occur in about half of these injuries and can play a role in determining the recommended treatment.
Nonsurgical Treatment
This treatment plan will progress from an initial focus on pain and swelling control through progressive physical therapy and rehabilitation. This may be supplemented with knee bracing. Many patients in this group will see a significant gain in function over the course of six to eight weeks, but full recovery can take several months. Some patients initially treated with nonsurgical means will find their knee to be too unstable and go on to have surgical treatment.
Surgical Treatment
The consensus on treating ACL tears surgically at this point is to reconstruct, rather than repair, the ACL. This means using a substitute graft made of tendon to replace the ACL. This graft can either come from another area of your own body, called an autograft, or from donated tissue, called an allograft. The choice of graft is often individualized based on associated injuries and surgeon and patient preference. Each option has its own pluses and minuses, but overall large studies show most grafts provide similar results in the long term.

The surgery will typically be performed with the assistance of small cameras, or arthroscopes, than can minimize the size of the incisions and aid in visualizing the joint. Most patients will go home the same day of their surgery. A brace may be used along with crutches to protect the repair in the early postoperative period. ACL surgery is very safe. Complications are rare but can include infection, bleeding, blood clots, stiffness, recurrent instability, and complications from harvesting tissue to replace your ACL.
Rehabilitation
While the surgery can often be the focus for many when dealing with an ACL tear, an equally important part is the rehabilitation. A combination of home exercises, formal physical therapy, and a return to full activity will take place over four to six months after ACL reconstruction. Crutches and bracing will be used in the first couple of weeks, and a period of restricted activity that may affect driving and certain job activities can be the norm. Long term, most patients will be able to return to their desired sport or other activity after going through this rehabilitation. If you or a family member is going through this injury, I hope everyone can use this information as a starting point to ask the right questions and feel comfortable starting down the road to getting back on the field!
What is your ACL?

How do I know if I tore it?
Most ACL tears will have the typical history above. I recommend anyone with that history to be evaluated by a physician in short time. That evaluation will focus on several things. First the stability of the knee will be tested on physical examination. This can also diagnose other ligament tears that can be associated with ACL tears. X-rays are helpful to rule out other injuries as well. Commonly this evaluation will result in an MRI, or magnetic resonance image, being ordered. This test, which does not involve radiation, will evaluate the soft tissue, cartilage, and bone of the knee with higher detail than an x-ray. When this information is available, your physician will be able to provide a complete diagnosis and treatment plan.

What’s Next?
At this point the treatment plan becomes very individualized. Every ACL tear is different in the amount of pain and instability a patient will suffer from. Different physical demands also go into determining the best way to treat a tear. In general, the younger and higher demand that a patient’s sport, job, or daily activities require, the more likely a surgical option is to be recommended. Associated injuries like meniscus and cartilage tears occur in about half of these injuries and can play a role in determining the recommended treatment.
Nonsurgical Treatment
This treatment plan will progress from an initial focus on pain and swelling control through progressive physical therapy and rehabilitation. This may be supplemented with knee bracing. Many patients in this group will see a significant gain in function over the course of six to eight weeks, but full recovery can take several months. Some patients initially treated with nonsurgical means will find their knee to be too unstable and go on to have surgical treatment.
Surgical Treatment
The consensus on treating ACL tears surgically at this point is to reconstruct, rather than repair, the ACL. This means using a substitute graft made of tendon to replace the ACL. This graft can either come from another area of your own body, called an autograft, or from donated tissue, called an allograft. The choice of graft is often individualized based on associated injuries and surgeon and patient preference. Each option has its own pluses and minuses, but overall large studies show most grafts provide similar results in the long term.

The surgery will typically be performed with the assistance of small cameras, or arthroscopes, than can minimize the size of the incisions and aid in visualizing the joint. Most patients will go home the same day of their surgery. A brace may be used along with crutches to protect the repair in the early postoperative period. ACL surgery is very safe. Complications are rare but can include infection, bleeding, blood clots, stiffness, recurrent instability, and complications from harvesting tissue to replace your ACL.
Rehabilitation
While the surgery can often be the focus for many when dealing with an ACL tear, an equally important part is the rehabilitation. A combination of home exercises, formal physical therapy, and a return to full activity will take place over four to six months after ACL reconstruction. Crutches and bracing will be used in the first couple of weeks, and a period of restricted activity that may affect driving and certain job activities can be the norm. Long term, most patients will be able to return to their desired sport or other activity after going through this rehabilitation. If you or a family member is going through this injury, I hope everyone can use this information as a starting point to ask the right questions and feel comfortable starting down the road to getting back on the field!
Wednesday, August 14, 2013
Suiting up with a new team: Dr. Abeln joins Floyd Memorial Hospital
When I began this blog I had hoped to post on a regular basis, and through the previous sports season was happy with the direction it was taking. Many posts discussed injuries affecting athletes, where changing teams comes with the territory. This scenario is increasingly becoming the norm in the medical field as well. As we head into the upcoming scholastic sports season I’m happy to announce I’ve been welcomed with open arms into the Floyd Memorial Medical Group, a team poised to lead the way in orthopedic care in the region. I will be joining Floyd Memorial Orthopedic Group in the upcoming weeks and couldn’t be more excited. Jumping across the river has opened numerous opportunities to service a thriving sports medicine scene in Southern Indiana while continuing to serve the community of Louisville and the rest of Kentuckiana.

Floyd Memorial Hospital in New Albany, Indiana has a stellar reputation in a range of services including orthopedics. I’m excited to join my new partners Drs. Mohammad Majd and Anifiok Uyoe in their New Albany location. This will allow this group to offer a wide range of orthopedic services, including spine, trauma, adult reconstruction, and sports medicine. Being a part of this team was a welcome opportunity that I could not be more excited to call my new home. As the season turns to fall I will be ramping up the number of posts and coverage of topics of interest to the sports medicine community that this blog covers. I hope the information proves useful and look forward to being a part of the team at my new home and interacting through this forum with athletes, patients, and the community at large. I've updated the scheduling link on this site and will officially begin my tenure on September 1st.

Floyd Memorial Hospital in New Albany, Indiana has a stellar reputation in a range of services including orthopedics. I’m excited to join my new partners Drs. Mohammad Majd and Anifiok Uyoe in their New Albany location. This will allow this group to offer a wide range of orthopedic services, including spine, trauma, adult reconstruction, and sports medicine. Being a part of this team was a welcome opportunity that I could not be more excited to call my new home. As the season turns to fall I will be ramping up the number of posts and coverage of topics of interest to the sports medicine community that this blog covers. I hope the information proves useful and look forward to being a part of the team at my new home and interacting through this forum with athletes, patients, and the community at large. I've updated the scheduling link on this site and will officially begin my tenure on September 1st.
Subscribe to:
Comments (Atom)