I've previously written on this space about ACL prevention. I wanted to update any readers that a new web site, sort of the next generation of the PEP program, has been unveiled. The FIFA 11+ program combines all the research of the PEP program and other ACL prevention strategies into a compact program meant to prevent a wide range of injuries, not just ACL tears. Check out more details and some great information at
FIFA 11+

Monday, December 2, 2013
Tuesday, November 26, 2013
Shoulder replacement, is it right for me?
Shoulder pain can be a debilitating condition. A range of issues can be the cause of this pain, from tendon and ligament tears that are more common in younger patients, to arthritis which more commonly affects middle-aged and older patients. Options for treating shoulder arthritis have increased dramatically in the last decade due to new technologies and research that has helped surgeons better understand the best approach to treating the various causes of shoulder pain in the older patient. Today I’d like to focus on that research, which predominantly involves shoulder arthroplasty, or replacement.

As in other joints in the body, the shoulder joint relies on smooth articular cartilage that lines the bones which form the joint. This smooth surface allows the shoulder to glide through a remarkable range of motion. If however the cartilage starts to thin out, those surfaces are no longer smooth. The human body will often react by forming bone spurs, or osteophytes, in an attempt to limit motion at this no longer smooth surface. This can result in further pain and loss of motion in the shoulder. At the same time, the muscles that stabilize the shoulder, the rotator cuff, can also be tearing. This can lead to further problems such as weakness in the shoulder, damage to the biceps tendon, and a special type of arthritis called rotator cuff arthropathy.

When this occurs, you will often notice pain, especially at night, in the shoulder. Motion will be lost, especially in attempting to reach overhead or behind your back. The shoulder may like it is grinding as well. If these symptoms are occurring the next step is to be seen in the office and evaluated by your surgeon. This will involve a physical exam and likely x-rays of the shoulder. In most cases of shoulder arthritis this is often enough testing to provide an accurate diagnosis and treatment plan. Sometimes an MRI or CT scan can be helpful for a more detailed assessment of the soft tissue and bony structure of the shoulder. Depending on the amount of cartilage loss and other damage to the shoulder, multiple treatment options exist. This can range from oral medications, ice, and physical therapy, to cortisone injections, to surgery.
The most predictable option to relieve arthritis of the shoulder joint is total joint replacement, or arthroplasty. This involves surgery to implant a combination and metal and plastic components that restore a smooth surface to the joint, improving motion and relieving pain. Standard arthroplasty is the most common option, with the newer reverse arthroplasty that I have displayed below an option for situations where there is a deficient rotator cuff. The surgery involves being placed under general anesthesia and several days stay in the hospital. After the replacement you can expect to wear a sling for 4-6 weeks and participate in physical therapy to focus on regaining motion and strength in the shoulder. Full recovery can take 3-4 months. Shoulder replacement surgery is highly successful. Risks of the surgery can involve infection, nerve injury, fracture, prosthesis related problems, and stiffness. Talk to your surgeon to discuss your specific condition and see if this surgery is an option for you.


As in other joints in the body, the shoulder joint relies on smooth articular cartilage that lines the bones which form the joint. This smooth surface allows the shoulder to glide through a remarkable range of motion. If however the cartilage starts to thin out, those surfaces are no longer smooth. The human body will often react by forming bone spurs, or osteophytes, in an attempt to limit motion at this no longer smooth surface. This can result in further pain and loss of motion in the shoulder. At the same time, the muscles that stabilize the shoulder, the rotator cuff, can also be tearing. This can lead to further problems such as weakness in the shoulder, damage to the biceps tendon, and a special type of arthritis called rotator cuff arthropathy.

When this occurs, you will often notice pain, especially at night, in the shoulder. Motion will be lost, especially in attempting to reach overhead or behind your back. The shoulder may like it is grinding as well. If these symptoms are occurring the next step is to be seen in the office and evaluated by your surgeon. This will involve a physical exam and likely x-rays of the shoulder. In most cases of shoulder arthritis this is often enough testing to provide an accurate diagnosis and treatment plan. Sometimes an MRI or CT scan can be helpful for a more detailed assessment of the soft tissue and bony structure of the shoulder. Depending on the amount of cartilage loss and other damage to the shoulder, multiple treatment options exist. This can range from oral medications, ice, and physical therapy, to cortisone injections, to surgery.
The most predictable option to relieve arthritis of the shoulder joint is total joint replacement, or arthroplasty. This involves surgery to implant a combination and metal and plastic components that restore a smooth surface to the joint, improving motion and relieving pain. Standard arthroplasty is the most common option, with the newer reverse arthroplasty that I have displayed below an option for situations where there is a deficient rotator cuff. The surgery involves being placed under general anesthesia and several days stay in the hospital. After the replacement you can expect to wear a sling for 4-6 weeks and participate in physical therapy to focus on regaining motion and strength in the shoulder. Full recovery can take 3-4 months. Shoulder replacement surgery is highly successful. Risks of the surgery can involve infection, nerve injury, fracture, prosthesis related problems, and stiffness. Talk to your surgeon to discuss your specific condition and see if this surgery is an option for you.

Tuesday, August 20, 2013
Expanding Team Coverage
I wanted to write today and thank the new schools that have offered to have me as part of their already excellent medical teams. I'll be working with a stellar group of doctors and trainers to provide orthopedic and sports medicine coverage at Jeffersonville, Clarksville, Providence, Charlestown, and North Harrison High Schools for the upcoming scholastic season. This is in addition to continuing my work with Indiana University Southeast, the University of Louisville, and Waggener High School. Providing care for scholastic athletes is one of the highlights of my career and I look forward to a successful and healthy season for all the competitors. Thanks to everyone at these institutions for having me as part of the team.
Thursday, August 15, 2013
I tore my ACL
The words above are amongst the most dreaded that can be spoken by any patient, be it a scholastic athlete, weekend warrior, or a work injury. Although the widespread attention this injury and its treatment have garnered from the coverage of college and professional athletes who have suffered it, there is often a significant amount of fear and uncertainty when dealing with the diagnosis, management, and recovery from this injury. The following post will go over this and hopefully provide a primer for patients and their families’ as they begin the road to recovery.
What is your ACL?
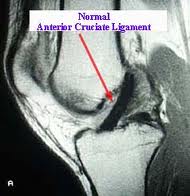
 The ACL, or anterior cruciate ligament, is one of four stabilizing ligaments of the knee. It is located within the knee joint and when torn, can leave the patient with the inability to perform activities that require cutting, pivoting, and a change of direction. Heavy lifting, climbing, and other job activities can be difficult as well. Walking, swimming, and other straight ahead and low impact activities are less often affected by this injury. ACL tears primarily occur via noncontact mechanisms. That is, an athlete will often be changing direction or landing when the injury occurs. These moments can be quite painful and patients will often feel or hear a pop, followed by rapid swelling of the knee and the inability to bear weight on the leg.
The ACL, or anterior cruciate ligament, is one of four stabilizing ligaments of the knee. It is located within the knee joint and when torn, can leave the patient with the inability to perform activities that require cutting, pivoting, and a change of direction. Heavy lifting, climbing, and other job activities can be difficult as well. Walking, swimming, and other straight ahead and low impact activities are less often affected by this injury. ACL tears primarily occur via noncontact mechanisms. That is, an athlete will often be changing direction or landing when the injury occurs. These moments can be quite painful and patients will often feel or hear a pop, followed by rapid swelling of the knee and the inability to bear weight on the leg.
How do I know if I tore it?
Most ACL tears will have the typical history above. I recommend anyone with that history to be evaluated by a physician in short time. That evaluation will focus on several things. First the stability of the knee will be tested on physical examination. This can also diagnose other ligament tears that can be associated with ACL tears. X-rays are helpful to rule out other injuries as well. Commonly this evaluation will result in an MRI, or magnetic resonance image, being ordered. This test, which does not involve radiation, will evaluate the soft tissue, cartilage, and bone of the knee with higher detail than an x-ray. When this information is available, your physician will be able to provide a complete diagnosis and treatment plan.


What’s Next?
At this point the treatment plan becomes very individualized. Every ACL tear is different in the amount of pain and instability a patient will suffer from. Different physical demands also go into determining the best way to treat a tear. In general, the younger and higher demand that a patient’s sport, job, or daily activities require, the more likely a surgical option is to be recommended. Associated injuries like meniscus and cartilage tears occur in about half of these injuries and can play a role in determining the recommended treatment.
Nonsurgical Treatment
This treatment plan will progress from an initial focus on pain and swelling control through progressive physical therapy and rehabilitation. This may be supplemented with knee bracing. Many patients in this group will see a significant gain in function over the course of six to eight weeks, but full recovery can take several months. Some patients initially treated with nonsurgical means will find their knee to be too unstable and go on to have surgical treatment.
Surgical Treatment
The consensus on treating ACL tears surgically at this point is to reconstruct, rather than repair, the ACL. This means using a substitute graft made of tendon to replace the ACL. This graft can either come from another area of your own body, called an autograft, or from donated tissue, called an allograft. The choice of graft is often individualized based on associated injuries and surgeon and patient preference. Each option has its own pluses and minuses, but overall large studies show most grafts provide similar results in the long term.

The surgery will typically be performed with the assistance of small cameras, or arthroscopes, than can minimize the size of the incisions and aid in visualizing the joint. Most patients will go home the same day of their surgery. A brace may be used along with crutches to protect the repair in the early postoperative period. ACL surgery is very safe. Complications are rare but can include infection, bleeding, blood clots, stiffness, recurrent instability, and complications from harvesting tissue to replace your ACL.
Rehabilitation
While the surgery can often be the focus for many when dealing with an ACL tear, an equally important part is the rehabilitation. A combination of home exercises, formal physical therapy, and a return to full activity will take place over four to six months after ACL reconstruction. Crutches and bracing will be used in the first couple of weeks, and a period of restricted activity that may affect driving and certain job activities can be the norm. Long term, most patients will be able to return to their desired sport or other activity after going through this rehabilitation. If you or a family member is going through this injury, I hope everyone can use this information as a starting point to ask the right questions and feel comfortable starting down the road to getting back on the field!
What is your ACL?

How do I know if I tore it?
Most ACL tears will have the typical history above. I recommend anyone with that history to be evaluated by a physician in short time. That evaluation will focus on several things. First the stability of the knee will be tested on physical examination. This can also diagnose other ligament tears that can be associated with ACL tears. X-rays are helpful to rule out other injuries as well. Commonly this evaluation will result in an MRI, or magnetic resonance image, being ordered. This test, which does not involve radiation, will evaluate the soft tissue, cartilage, and bone of the knee with higher detail than an x-ray. When this information is available, your physician will be able to provide a complete diagnosis and treatment plan.

What’s Next?
At this point the treatment plan becomes very individualized. Every ACL tear is different in the amount of pain and instability a patient will suffer from. Different physical demands also go into determining the best way to treat a tear. In general, the younger and higher demand that a patient’s sport, job, or daily activities require, the more likely a surgical option is to be recommended. Associated injuries like meniscus and cartilage tears occur in about half of these injuries and can play a role in determining the recommended treatment.
Nonsurgical Treatment
This treatment plan will progress from an initial focus on pain and swelling control through progressive physical therapy and rehabilitation. This may be supplemented with knee bracing. Many patients in this group will see a significant gain in function over the course of six to eight weeks, but full recovery can take several months. Some patients initially treated with nonsurgical means will find their knee to be too unstable and go on to have surgical treatment.
Surgical Treatment
The consensus on treating ACL tears surgically at this point is to reconstruct, rather than repair, the ACL. This means using a substitute graft made of tendon to replace the ACL. This graft can either come from another area of your own body, called an autograft, or from donated tissue, called an allograft. The choice of graft is often individualized based on associated injuries and surgeon and patient preference. Each option has its own pluses and minuses, but overall large studies show most grafts provide similar results in the long term.

The surgery will typically be performed with the assistance of small cameras, or arthroscopes, than can minimize the size of the incisions and aid in visualizing the joint. Most patients will go home the same day of their surgery. A brace may be used along with crutches to protect the repair in the early postoperative period. ACL surgery is very safe. Complications are rare but can include infection, bleeding, blood clots, stiffness, recurrent instability, and complications from harvesting tissue to replace your ACL.
Rehabilitation
While the surgery can often be the focus for many when dealing with an ACL tear, an equally important part is the rehabilitation. A combination of home exercises, formal physical therapy, and a return to full activity will take place over four to six months after ACL reconstruction. Crutches and bracing will be used in the first couple of weeks, and a period of restricted activity that may affect driving and certain job activities can be the norm. Long term, most patients will be able to return to their desired sport or other activity after going through this rehabilitation. If you or a family member is going through this injury, I hope everyone can use this information as a starting point to ask the right questions and feel comfortable starting down the road to getting back on the field!
Wednesday, August 14, 2013
Suiting up with a new team: Dr. Abeln joins Floyd Memorial Hospital
When I began this blog I had hoped to post on a regular basis, and through the previous sports season was happy with the direction it was taking. Many posts discussed injuries affecting athletes, where changing teams comes with the territory. This scenario is increasingly becoming the norm in the medical field as well. As we head into the upcoming scholastic sports season I’m happy to announce I’ve been welcomed with open arms into the Floyd Memorial Medical Group, a team poised to lead the way in orthopedic care in the region. I will be joining Floyd Memorial Orthopedic Group in the upcoming weeks and couldn’t be more excited. Jumping across the river has opened numerous opportunities to service a thriving sports medicine scene in Southern Indiana while continuing to serve the community of Louisville and the rest of Kentuckiana.

Floyd Memorial Hospital in New Albany, Indiana has a stellar reputation in a range of services including orthopedics. I’m excited to join my new partners Drs. Mohammad Majd and Anifiok Uyoe in their New Albany location. This will allow this group to offer a wide range of orthopedic services, including spine, trauma, adult reconstruction, and sports medicine. Being a part of this team was a welcome opportunity that I could not be more excited to call my new home. As the season turns to fall I will be ramping up the number of posts and coverage of topics of interest to the sports medicine community that this blog covers. I hope the information proves useful and look forward to being a part of the team at my new home and interacting through this forum with athletes, patients, and the community at large. I've updated the scheduling link on this site and will officially begin my tenure on September 1st.

Floyd Memorial Hospital in New Albany, Indiana has a stellar reputation in a range of services including orthopedics. I’m excited to join my new partners Drs. Mohammad Majd and Anifiok Uyoe in their New Albany location. This will allow this group to offer a wide range of orthopedic services, including spine, trauma, adult reconstruction, and sports medicine. Being a part of this team was a welcome opportunity that I could not be more excited to call my new home. As the season turns to fall I will be ramping up the number of posts and coverage of topics of interest to the sports medicine community that this blog covers. I hope the information proves useful and look forward to being a part of the team at my new home and interacting through this forum with athletes, patients, and the community at large. I've updated the scheduling link on this site and will officially begin my tenure on September 1st.
Wednesday, June 19, 2013
Platelet Rich Plasma. Understanding PRP's Role in Sports Medicine
Platelet rich plasma, or PRP, has gained increasing use in treating musculoskeletal injuries in the past decade. Several high profile uses in professional athletes have led to its widespread application in the general public, and an explosion of research into its utility. Today’s entry will hopefully provide an understanding of where we stand with PRP, its function, and the role for its use in treating sports medicine injuries today.
What is PRP?
PRP at its most basic form is any blood product with a concentration of platelets above normal concentration. Platelets are a cellular component of blood that have a role in tissue healing and blood clotting. It’s their role in tissue healing that has spawned its use in a range of therapeutic applications including sports medicine. By increasing the concentration of platelets, PRP systems also increase the concentration of the important growth factors these cells release, providing a product shown to enhance healing of musculoskeletal tissue.

PRP is obtained with a simple blood draw, often in your physician office. It is then processed in a centrifuge to concentrate platelet cells and separate out other cells and fluids. It is then injected in the injured tissue or joint after a local anesthetic is applied. A short period of rest is often recommended to minimize the chances of pain at the injection site and to allow the healing process to begin.

What do we treat with PRP?
A number of clinical studies have been released in recent years looking at PRP’s utility in a range of conditions, from arthritis to acute muscle and ligament injuries to chronic conditions like tendonitis and plantar fasciitis. Further studies have looked into its role in augmenting surgical repair of the structures such as the rotator cuff, achilles tendon, and anterior cruciate ligament. Broadly speaking, these studies would indicate that PRP’s efficacy is best classified as mixed. Many of these studies are relatively small and often conflict with one another. The clearest benefit for the use of PRP has been its use in treating lateral epicondylitis, or tennis elbow, plantar fasciitis, and osteoarthritis of the knee. Its usefulness in treating acute injuries, patellar tendonitis, hip bursitis, and in augmenting surgical repairs is mixed at best, and in the case of rotator cuff repair may even be detrimental to healing.

Should I get a PRP injection?
That is often the question most patients want answered. The clearest answer is to talk to your physician. He or she should be able to discuss PRP’s use in your specific condition. Often other remedies such as physical therapy, rest, or braces can offer a more reliable cure. However, certain conditions do appear to be better candidates for PRP, and I have found it to be very useful for the patient who has tried and failed more traditional approaches such as steroid injections, prolonged physical therapy, and rest. An individualized approach to these conditions is certainly the best medicine.
What is PRP?
PRP at its most basic form is any blood product with a concentration of platelets above normal concentration. Platelets are a cellular component of blood that have a role in tissue healing and blood clotting. It’s their role in tissue healing that has spawned its use in a range of therapeutic applications including sports medicine. By increasing the concentration of platelets, PRP systems also increase the concentration of the important growth factors these cells release, providing a product shown to enhance healing of musculoskeletal tissue.

PRP is obtained with a simple blood draw, often in your physician office. It is then processed in a centrifuge to concentrate platelet cells and separate out other cells and fluids. It is then injected in the injured tissue or joint after a local anesthetic is applied. A short period of rest is often recommended to minimize the chances of pain at the injection site and to allow the healing process to begin.

What do we treat with PRP?
A number of clinical studies have been released in recent years looking at PRP’s utility in a range of conditions, from arthritis to acute muscle and ligament injuries to chronic conditions like tendonitis and plantar fasciitis. Further studies have looked into its role in augmenting surgical repair of the structures such as the rotator cuff, achilles tendon, and anterior cruciate ligament. Broadly speaking, these studies would indicate that PRP’s efficacy is best classified as mixed. Many of these studies are relatively small and often conflict with one another. The clearest benefit for the use of PRP has been its use in treating lateral epicondylitis, or tennis elbow, plantar fasciitis, and osteoarthritis of the knee. Its usefulness in treating acute injuries, patellar tendonitis, hip bursitis, and in augmenting surgical repairs is mixed at best, and in the case of rotator cuff repair may even be detrimental to healing.

Should I get a PRP injection?
That is often the question most patients want answered. The clearest answer is to talk to your physician. He or she should be able to discuss PRP’s use in your specific condition. Often other remedies such as physical therapy, rest, or braces can offer a more reliable cure. However, certain conditions do appear to be better candidates for PRP, and I have found it to be very useful for the patient who has tried and failed more traditional approaches such as steroid injections, prolonged physical therapy, and rest. An individualized approach to these conditions is certainly the best medicine.
Tuesday, February 12, 2013
Meniscus Tear Part Two: Treatment Options
In part one of my post on meniscus tears, I discussed the role of the meniscus in knee function, ways it can be injured, symptoms of a tear, and tests and exams a physician can use to diagnose them. Once that is established, the discussion quickly turns to how best treat these tears.
The most important thing I emphasize with patients is that every meniscus tear is different. There are many things to consider when discussing the best treatment option. The location and type of tear, the patient’s age and activity level, associated symptoms such as if the knee is locking or not, and the presence of other conditions such as osteoarthritis and ligament tears are all important considerations in choosing the best way to proceed
Nonoperative Options
The broadest way to break down treatment options is whether the tear will be treated with or without surgery. With this in mind, there are several instances where most patients will be recommended to not consider nonoperative options. If the knee is locked because of certain meniscus tears, nonoperative treatment is unlikely to lead to successful results. Worst still, the locked fragment can damage the articular surface of the joint if left for too long. Further, meniscus tears associated with significant ligament injuries such as ACL, or anterior cruciate ligament, in athletes or those requiring full stability of their knee will often have their meniscus tear treated surgically at the same time as their ligament tear.
So, for those tears not meeting those criteria, what can be done to hopefully avoid a trip to the operating room? Conservative options abound for many types of meniscus tears, especially smaller degenerative type tears associated with arthritis. Rest, ice, anti-inflammatory medication, and physical therapy can decrease the pain and swelling associated with these tears. Corticosteroid injections have been utilized for years and can be effective if these first line treatments fail to relieve your pain. Newer medications and treatments, such as viscosupplementation and PRP, or platelet rich plasma, are not as well studied but are being increasingly used in the conservative management of certain types of meniscus tears. Each of these can be performed in the physician office with minimal down time. I’ve found nonoperative approaches to be most successful in patients who have few mechanical complaints, that it catching or locking of the knee, or a sensation of popping with activities.

Operative Options
For patients who have failed conservative approaches or have more significant symptoms, surgery can offer relief that can allow you to return to the activities that sports, your job, and life demand. Meniscus tears are now treated almost exclusively via arthroscopic surgery. This surgery utilizes small incisions and instruments the size of a pencil and smaller to assess the tear and manage it.

During surgery, meniscus tears can be addressed one of two ways. The tissue will either be sewed back together, or repaired, or more commonly, trimmed out to remove the damaged tissue that is causing pain. Meniscus repairs are much less common because there are few tears that meet the criteria for this type of treatment. Factors such as your age, the type and location of the tear, the quality of the tissue, and the presence of arthritis are all factors your physician should discuss as before surgery. The final determination of whether the meniscus can be repaired or not will occur during surgery. If it can be repaired, a variety of options exist. Suture can be placed into the meniscus through the same arthroscopic incisions, or through needles placed through the skin. Some tears are better treated by making incisions on the side of the knee to more safely and securely pass the sutures. Meniscus repair requires prolonged rehabilitation, often with crutches, bracing, and periods of nonweightbearing and physical therapy to allow the meniscus to heal.

The more common approach of trimming out the damaged tissue, or partial meniscectomy, does not require the same precautions as a meniscus repair, yet still requires a period of rest and often physical therapy to allow a full recovery. Crutches or a cane can allow the knee to rest for a short period of time after surgery, and limiting how much walking and other activities one does will minimize swelling that can slow down the rehabilitation process

Recognizing that a variety of options exist in treating your meniscus tear is the first step in obtaining a successful outcome. A range of treatments can typically be offered and the first step does not always have to be surgery. If surgery is chosen, most patients will reach a full recovery and have the chance to return to all levels of previous activity. Talk to your physician about your individual case and find what works for you.
The most important thing I emphasize with patients is that every meniscus tear is different. There are many things to consider when discussing the best treatment option. The location and type of tear, the patient’s age and activity level, associated symptoms such as if the knee is locking or not, and the presence of other conditions such as osteoarthritis and ligament tears are all important considerations in choosing the best way to proceed
Nonoperative Options
The broadest way to break down treatment options is whether the tear will be treated with or without surgery. With this in mind, there are several instances where most patients will be recommended to not consider nonoperative options. If the knee is locked because of certain meniscus tears, nonoperative treatment is unlikely to lead to successful results. Worst still, the locked fragment can damage the articular surface of the joint if left for too long. Further, meniscus tears associated with significant ligament injuries such as ACL, or anterior cruciate ligament, in athletes or those requiring full stability of their knee will often have their meniscus tear treated surgically at the same time as their ligament tear.
So, for those tears not meeting those criteria, what can be done to hopefully avoid a trip to the operating room? Conservative options abound for many types of meniscus tears, especially smaller degenerative type tears associated with arthritis. Rest, ice, anti-inflammatory medication, and physical therapy can decrease the pain and swelling associated with these tears. Corticosteroid injections have been utilized for years and can be effective if these first line treatments fail to relieve your pain. Newer medications and treatments, such as viscosupplementation and PRP, or platelet rich plasma, are not as well studied but are being increasingly used in the conservative management of certain types of meniscus tears. Each of these can be performed in the physician office with minimal down time. I’ve found nonoperative approaches to be most successful in patients who have few mechanical complaints, that it catching or locking of the knee, or a sensation of popping with activities.

Operative Options
For patients who have failed conservative approaches or have more significant symptoms, surgery can offer relief that can allow you to return to the activities that sports, your job, and life demand. Meniscus tears are now treated almost exclusively via arthroscopic surgery. This surgery utilizes small incisions and instruments the size of a pencil and smaller to assess the tear and manage it.

During surgery, meniscus tears can be addressed one of two ways. The tissue will either be sewed back together, or repaired, or more commonly, trimmed out to remove the damaged tissue that is causing pain. Meniscus repairs are much less common because there are few tears that meet the criteria for this type of treatment. Factors such as your age, the type and location of the tear, the quality of the tissue, and the presence of arthritis are all factors your physician should discuss as before surgery. The final determination of whether the meniscus can be repaired or not will occur during surgery. If it can be repaired, a variety of options exist. Suture can be placed into the meniscus through the same arthroscopic incisions, or through needles placed through the skin. Some tears are better treated by making incisions on the side of the knee to more safely and securely pass the sutures. Meniscus repair requires prolonged rehabilitation, often with crutches, bracing, and periods of nonweightbearing and physical therapy to allow the meniscus to heal.

The more common approach of trimming out the damaged tissue, or partial meniscectomy, does not require the same precautions as a meniscus repair, yet still requires a period of rest and often physical therapy to allow a full recovery. Crutches or a cane can allow the knee to rest for a short period of time after surgery, and limiting how much walking and other activities one does will minimize swelling that can slow down the rehabilitation process

Recognizing that a variety of options exist in treating your meniscus tear is the first step in obtaining a successful outcome. A range of treatments can typically be offered and the first step does not always have to be surgery. If surgery is chosen, most patients will reach a full recovery and have the chance to return to all levels of previous activity. Talk to your physician about your individual case and find what works for you.
Tuesday, February 5, 2013
Meniscus Tears Part One
The human knee joint can take a tremendous toll in the course of athletic participation, with injury, even everyday activities. A force of three to six times one’s body weight is transmitted through the knee every step one takes. To spread that load and lessen damage to the joint, we rely on a structure called the meniscus, semicircular bands of tissue spanning each side of the joint which service to distribute load and stabilize the knee.

Meniscus tears can occur in a variety of settings. Athletic injury, work accidents, and even minor trauma to the knee can cause acute tears. Age related changes often result in chronic or degenerative tears, of the meniscus which can commonly be seen in the setting of osteoarthritis.

Typical symptoms of a meniscus tear include pain, swelling, and sometimes a sensation of a pop when it occurs. Other associated symptoms can include locking or catching of the knee, a feeling of giving way, and a loss of range of motion

When these symptoms are present, a thorough physical examination is the first step for you and your physician. X-rays can be helpful to evaluate for other conditions such as a fracture, or more commonly osteoarthritis. Magnetic resonance imaging, or an MRI, can fully evaluate the soft tissues of the knee including the meniscus.


Meniscus tears can occur in a variety of settings. Athletic injury, work accidents, and even minor trauma to the knee can cause acute tears. Age related changes often result in chronic or degenerative tears, of the meniscus which can commonly be seen in the setting of osteoarthritis.

Typical symptoms of a meniscus tear include pain, swelling, and sometimes a sensation of a pop when it occurs. Other associated symptoms can include locking or catching of the knee, a feeling of giving way, and a loss of range of motion

When these symptoms are present, a thorough physical examination is the first step for you and your physician. X-rays can be helpful to evaluate for other conditions such as a fracture, or more commonly osteoarthritis. Magnetic resonance imaging, or an MRI, can fully evaluate the soft tissues of the knee including the meniscus.

Sunday, January 6, 2013
Guidelines for healthy marathon running
Marathon running has seen a surge in popularity, with participants nationwide nearly doubling in the last decade. This has brought a new crop of runners into the fold and with it unfortunately exposure to high rates of injury. Running-related injuries, or RRI, can be seen in upwards of three quarters of participants in training cycles for distance running events. One size fits all approaches previously geared to experienced runners have traditionally been the norm in training programs for marathons. While serving as a nice framework, more general guidelines as well as alternative means of training may be more appropriate for novice runners. They can also prove useful for more experienced athletes when injuries do occur during training.


The first consideration is what to do before one starts training. An argument could be made that a thorough physical exam and any indicated testing including an EKG should precede training for a marathon or half marathon. 59 cardiac deaths occurred in the US during the previous decade. Hypertrophic cardiomyopathy, coronary artery disease, and male gender were the overwhelming risk factors. I advise any participant with a family history of these two risk factors, and men over the age of 35 to have thorough history and physical before training begins. Further, I highly encourage runners and their training partners/friend/family to learn CPR. Early administration of CPR resulted in higher survival rates in these athletes. Lastly, seek medical attention for any symptoms of heart disease such as chest pain, shortness of breath, or lightheadedness.

Proper equipment should be a runner’s next step. Several properly fitting shoes, which the experts at local running stores can be of tremendous help, should be a mandatory purchase. Gaining adequate correction of any pronation or arch issues should start there as well. Most guidelines suggest running shoes should be replaced every 350-500 miles. Every runner is different though. Increasing aches and pains, signs of midsole wear, and significant tread wear should prompt a trip to the running store.
Finally it’s time to train. Many marathon and half marathons, running magazines, and other sources now provide day by day training calendars. They’re available on multiple platforms, from traditional print, to web, and now smartphone capability. They can provide structure and help plan the when, how much, and how long for your training runs. I think most of them are done quite well so will delve into what I think are good, general guidelines for athletes in distance events. My general recommendations are to gradually increase mileage until two weeks prior to the race. During that time two long runs a week should gradually build until that run is 18-20 miles. Shorter runs in between should be in the 4-6 mile range. Perform interval training one day a week with short distances or short mixed into an overall shorter run. Run a maximum of six days a week. A day of total rest will allow recovery. Stretching, warming up, cooling down, and icing should be a part of any runner’s routine.
 Within that guideline, I think there is tremendous room for modification to prevent injury. Alternating surfaces to dirt and grass is a start. Skipping a light day of running for alternative aerobic activity like swimming, cycling, and elliptical training can ease aches and pains. Pool running can allow you to continue working on your form and cadence, while taking pressure off of joints and providing added resistance training.
Within that guideline, I think there is tremendous room for modification to prevent injury. Alternating surfaces to dirt and grass is a start. Skipping a light day of running for alternative aerobic activity like swimming, cycling, and elliptical training can ease aches and pains. Pool running can allow you to continue working on your form and cadence, while taking pressure off of joints and providing added resistance training.

Lastly nutrition is critical to successfully training and competing in distance events. Everyday training will require an increase in caloric intake above average intake. Protein intake of a gram per body weight is often recommended. Maintaining an overall well rounded diet rich in fruits and vegetables will prove beneficial. During competition, carbohydrates are your primary fuel source. Thus the ubiquitous carb-loading pre-race pasta meal. Two recent studies looking at participants in the Eau Claire and London Marathons showed better performance amongst participants who had carb-loaded 24-36 hours pre-race. The authors defined carb-loading as greater than 7 grams of carbohydrates for every gram of body weight. The morning of the race, simple carbs like toast, oatmeal, and bagels. Go low on proteins as they can take too long to digest. Many runners like to throw in a banana for its potassium. After that, hydrate, and good luck!


The first consideration is what to do before one starts training. An argument could be made that a thorough physical exam and any indicated testing including an EKG should precede training for a marathon or half marathon. 59 cardiac deaths occurred in the US during the previous decade. Hypertrophic cardiomyopathy, coronary artery disease, and male gender were the overwhelming risk factors. I advise any participant with a family history of these two risk factors, and men over the age of 35 to have thorough history and physical before training begins. Further, I highly encourage runners and their training partners/friend/family to learn CPR. Early administration of CPR resulted in higher survival rates in these athletes. Lastly, seek medical attention for any symptoms of heart disease such as chest pain, shortness of breath, or lightheadedness.

Proper equipment should be a runner’s next step. Several properly fitting shoes, which the experts at local running stores can be of tremendous help, should be a mandatory purchase. Gaining adequate correction of any pronation or arch issues should start there as well. Most guidelines suggest running shoes should be replaced every 350-500 miles. Every runner is different though. Increasing aches and pains, signs of midsole wear, and significant tread wear should prompt a trip to the running store.
Finally it’s time to train. Many marathon and half marathons, running magazines, and other sources now provide day by day training calendars. They’re available on multiple platforms, from traditional print, to web, and now smartphone capability. They can provide structure and help plan the when, how much, and how long for your training runs. I think most of them are done quite well so will delve into what I think are good, general guidelines for athletes in distance events. My general recommendations are to gradually increase mileage until two weeks prior to the race. During that time two long runs a week should gradually build until that run is 18-20 miles. Shorter runs in between should be in the 4-6 mile range. Perform interval training one day a week with short distances or short mixed into an overall shorter run. Run a maximum of six days a week. A day of total rest will allow recovery. Stretching, warming up, cooling down, and icing should be a part of any runner’s routine.


Lastly nutrition is critical to successfully training and competing in distance events. Everyday training will require an increase in caloric intake above average intake. Protein intake of a gram per body weight is often recommended. Maintaining an overall well rounded diet rich in fruits and vegetables will prove beneficial. During competition, carbohydrates are your primary fuel source. Thus the ubiquitous carb-loading pre-race pasta meal. Two recent studies looking at participants in the Eau Claire and London Marathons showed better performance amongst participants who had carb-loaded 24-36 hours pre-race. The authors defined carb-loading as greater than 7 grams of carbohydrates for every gram of body weight. The morning of the race, simple carbs like toast, oatmeal, and bagels. Go low on proteins as they can take too long to digest. Many runners like to throw in a banana for its potassium. After that, hydrate, and good luck!
Subscribe to:
Comments (Atom)